Long case final practical -1701006006
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs. This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box
A 30 year old female patient who is house wife by occupation resident of Nalgonda came to OPD with chief complaints of
Chief complaints :
Abdominal pain since 2 days
Facial puffiness and pedal Edema since 2 days
Shortness of breath since 2 days
History of presenting illness :
Patient was asymptomatic 12 months back and she developed facial puffiness and bilateral leg swelling which was pitting in type
SOB: insidious in onset gradually progressed to grade 4 not associated with change in position no aggravating and relieving factors
Abdominal pain : pain since 2 days which started suddenly and burning type of pain
In epigastric region
No aggravating and reliving factors
Past history
She is a known case of hypertension since 12 years 

Personal history :
Appetite : decreased
Diet : mixed
Sleep : inadequate
Bladder : decreased urine output
Bowel movements: regular
Addictions :absent
Family history:
Patients mother is hypertensive
General examination:
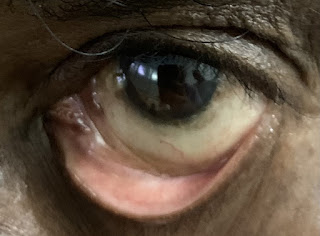
Pallor: present
Icterus: absent
Cyanosis : absent
Clubbing : absent
Lymphadenopathy : absent
Edema : absent





Vitals:
Temperature: a febrile
Pulse: 120bpm
Blood pressure:150/90 mm of hg
Respiratory rate : 34 bpm
Systemic examination:
Cardiovascular system
JVP -raised
Visible pulsations: absent
Apical impulse : shifted downward and laterally 6th intercostal space
Thrills -absent
S1, S2 - heart sounds muffled
Pericardial rub -present
Respiratory system:
Patient examined in sitting position
Inspection:-
oral cavity- Normal ,nose- normal ,pharynx-normal
Shape of chest - normal
Chest movements : bilaterally symmetrically reduced
Trachea is central in position & Nipples are in 4th Intercoastal space
Palpation:-
All inspiratory findings are confirmed
Trachea central in position
Apical impulse in left 6 thICS,
Chest movements bilaterally symmetrical reduced
Tactile and vocal fremitus reduced on both sides in infra axillary and infra scapular region
PERCUSSION
DULL IN BOTH SIDESIN
AUSCULTATION DECREASED ON BOTH SIDE
bronchial sounds are heared -reduced
Abdomen examination:
INSPECTION
Shape : distended
Umbilicus:normal
Movements :normal
Visible pulsations :absent
Skin or surface of the abdomen : normal
PALPATION
Liver is not palpable
PERCUSSION- dull
AUSCULTATION :bowel sounds heard




PLEURAL TAP



















PROVISIONAL DIAGNOSIS:
CKD on MHD
Treatment:
INJ. MONOCEF 1gm/IV/BD
INJ. METROGYL 100ml/IV/TID
INJ PAN 40mg/IV/OD
INJ. ZOFER 4mg/iv/SOS
TAB. LASIX 40mg/PO/BD
TAB. NICORANDIL 20mg/PO/TID
INJ. BUSOCOPAN /iv/stat
Add on
TAB. OROFER PO/BD
TAB. NODOSIS 500mg/PO/TID
INJ.EPO 4000 ml/ weekly
TAB. SHELLCAL/PO/BD
DIALYSIS (HD)
INJ.KCL 2AMP IN 500 ml NS over 5min
Comments
Post a Comment