54 year old female
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs. This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box
Consumes mixed diet
Appetite reduced
Bowel n bladder regular
Sleep adequate
BP-120/80 mm of Hg
PR-67/min
RR-20/min
afebrile
SYSTEMIC EXAMINATION
CVS:S1S2 heard
Jvp not raised
No murmurs heard
RESPIRATORY: BAE+, clear
ABDOMEN: Soft, non tender, BS+, no organomegaly.
CNS: NFND.
Course in the hospital
A 54-year female clinically presented to the causality with the above-mentioned complaints. Upon admission, necessary investigations were done. Her initial workup showed Hb 13.1 gm/dl; TLC 8600 cells/mm³; platelet count 1 lakhs/mm³. She had a lesion over the right infra axillary region for which use was advised. She had postural drop for which intravenous fluid resuscitation and replacement with meticulous monitoring was done.
2D ECHO was done on 15/9/22 which showed evidence of :
Good LV systolic function with Ejection fraction of 60% ; No RWMA; No MS or AS; Trivial TR and AR; No MR; Minimal pericardial effusion; Diastolic dysfunction was present; IVC size of 1.3 cms; No LV clots.
On 16/09/2022 her Hb was 14.6 gm/dl; TLC 9900 cells/mm³; platelet count 1 lakhs/mm³.
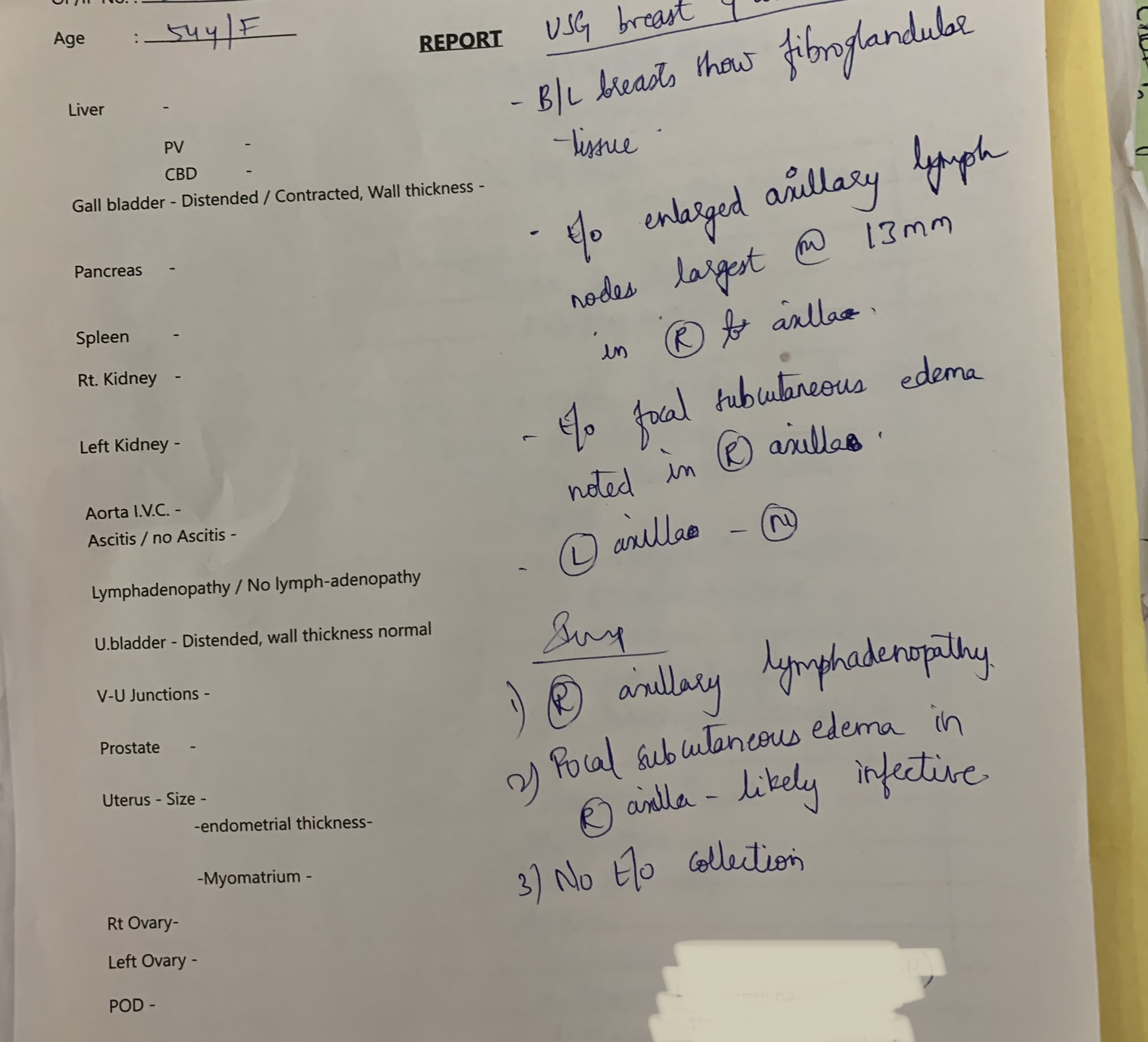
On16/09/22 ultrasound breast and axilla was done which showed Right axillary lymphadenopathy and Focal subcutaneous edema in right axilla- likely infective
On 17/09/2022 her Hb was 13.2 gm/dl
TLC 10,300 cells/mm³.platelet count 40,000 lakhs/mm³. She has been advised to have plenty of oral fluids. She was tolerating feeds well but has residual symptoms like nausea, generalised weakness and decreased appetite. During the stay in hospital she was treated with IV Fluids, Antibiotics, Antipyretics and supportive medications . On 18:09/2022 her Hb was 13.3 gm/dl, TLC 10,400 cells/mm³, platelet count 1.93 lakhs/mm³. Her condition was gradually improved and discharged in a stable condition.










INVESTIGATIONS



1. IVF NS/RL @75ML/HOUR2. INJ. NEOMOL 100ML /IV/SOS3. TAB. DOLO 650MG/PO/QID.4.OPTINEURON 1AMP in 100 ml /NS/IV/OD5.TAB LIMCEE50mg/PO/OD6.tab.DOXY 100 mg BD7.INJ.MONOCEF1gm/IV/BD
8.TAB. METFORMIN 500mg /PO/OD
9.temperature and vital monitoring
Comments
Post a Comment